DEVELOPMENT IN A LABOR AND DELIVERY UNIT
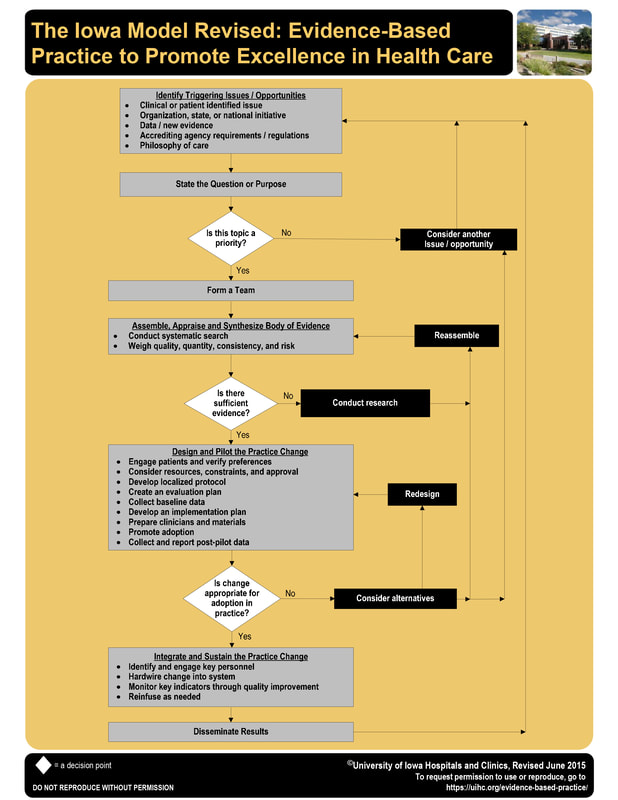
In order to implement a formal debriefing program in a labor and delivery unit, The Iowa Model Revised: Evidence-Based Practice to Promote Excellence in Health Care was followed.
First, the clinical issue was identified and the purpose was stated in PICO form.

Patient Population
Clinical Problem
Pilot area
Intervention
Comparison
Anticipated Outcomes
- OB team (nurses, obstetricians, anesthesiologists, surgical technicians, unit coordinators, laboratory, blood bank, nursing supervisors, transporters, and all members of the care team)
Clinical Problem
- OB team does not debrief after critical obstetric events.
Pilot area
- Labor and Delivery, limited to the day shift when the evidence-based practice nurse (debriefing champion) is working.
Intervention
- OB team debriefs as close to the critical event as possible; maximum of fifteen minute session before the end of the shift.
Comparison
- Debriefing does not occur when the evidence-based practice nurse (debriefing champion) is not working.
Anticipated Outcomes
- Transparency, improved team functioning and communication, just culture, improved systems, improved patient care, and a highly reliable, empowered OB team
In this model, the next question is, “is this topic a priority?” If the answer if yes, one continues with the model.
If the topic is a priority, the next step is to form a team.

As a Masters of Nursing student, the debriefing champion did not form a team, but continued on to the next step in the model.

A systematic literature search with the use of electronic databases including PubMed, CINAHL, and Clinical Key for Nursing was completed. Search words included labor and delivery, nurse facilitated debriefing, and team dynamics. The clinical debriefing literature was assembled, appraised, and synthesized. Articles about critical incident stress debriefing were excluded from the review.
Once the literature search is complete, the Iowa Model asks, “is there sufficient evidence?” There was sufficient evidence about the value of clinical debriefing, but the debriefing program was not implemented in the clinical unit until the debriefing champion was sponsored by the Association of Women’s Health, Obstetric, and Neonatal Nurses (AWHONN) to attend the University of Iowa Advanced Practice Institute (API): Promoting Adoption of Evidence-Based Practice.
The next step in Iowa Model instructs the nurse scientist to design and pilot the practice change. This step includes developing a localized protocol, developing implementation and evaluation plans, preparing materials, collecting baseline data, promoting adoption, and collecting and reporting post-pilot data. This was the focus while attending the API in Iowa.
The debriefing champion created a double sided debriefing tool to serve as a script and guide to facilitate a clinical debrief. The facilitators were asked to use the script to initiate and conclude each debrief. The script is important to ensure that people are thanked for their time and that the most important elements of the program are highlighted.
The debriefing champion created a double sided debriefing tool to serve as a script and guide to facilitate a clinical debrief. The facilitators were asked to use the script to initiate and conclude each debrief. The script is important to ensure that people are thanked for their time and that the most important elements of the program are highlighted.
- Confidentiality
- Just culture
- INFO debrief



In addition, the Iowa evidence-based practice experts emphasized the value of forming a team, an essential step that was missed early in the model, so the formation of a team of clinicians with the ability to positively influence their peers was paramount upon return to the clinical unit. The debriefing champion engaged with the institution's research institute to obtain Institutional Review Board approval to collect baseline data about clinicians’ knowledge, skills, and attitudes about debriefing after critical obstetric events. The research professionals also collaborated to develop a plan about how to collect and evaluate data at meaningful points over the course of one year. Then, a team from the Organizational Development Department joined the team to create a SurveyMonkey as a tool collect the desired data. This survey was electronically distributed to the labor and delivery and Neonatal Intensive Care Unit staff, including physicians, nurses, respiratory therapists, and technicians. The survey was also distributed to the hospital's contracted group of anesthesia physicians.
The unit based debriefing team developed the BeeBrief logo to create interest and awareness in the program. Every time there is a clinical debrief, a staff member writes the date on this image, and posts it on a bulletin board in the nurse's lounge. The goal is to acknowledge that the unit has debriefed while respecting confidentiality.

While it was evident from the literature search that there was sufficient evidence to support this practice change, limited details about implementing clinical debriefing programs were available. One model for a clinical debriefing program was shared by Stuart Rose and Adam Cheng (2018) in their article, Charge Nurse Facilitated Debriefing in the Emergency Department. In this article, the authors described how the INFO debrief (Immediate, Not for personal assessment, Fast facilitated feedback and Opportunity to ask questions) established a process for charge nurses to facilitate clinical debriefs immediately after resuscitations. While the emergency department and labor and delivery units are not identical, the INFO debrief model, with modifications, could be applicable for use in the obstetric unit. Written permission to use the INFO pneumonic was obtained via email communication with Dr. Rose.
Modeled after the emergency room clinical debriefing program, charge nurses were identified as the clinical debriefing champions. Each charge nurse was expected to attend a mandatory one hour training session; multiple training sessions were offered during a two week time period. The training session included a PowerPoint presentation to introduce the background of debriefing, the evidence for debriefing, and goals of debriefing. The concepts of high reliability and just culture were established. Facilitation skills were discussed, including how to carefully select words, tone of voice, and body language to ensure that participants feel safe. The INFO pneumonic was discussed at length. A detailed discussion about how to use the debriefing tool was part of the training.
I is for immediately after an event
Modeled after the emergency room clinical debriefing program, charge nurses were identified as the clinical debriefing champions. Each charge nurse was expected to attend a mandatory one hour training session; multiple training sessions were offered during a two week time period. The training session included a PowerPoint presentation to introduce the background of debriefing, the evidence for debriefing, and goals of debriefing. The concepts of high reliability and just culture were established. Facilitation skills were discussed, including how to carefully select words, tone of voice, and body language to ensure that participants feel safe. The INFO pneumonic was discussed at length. A detailed discussion about how to use the debriefing tool was part of the training.
I is for immediately after an event
- Try to gather the team as soon as possible as more team members are available and recall bias is limited
- This involves a change in the culture with buy in from the entire labor and delivery team
- A nurse may be asked to step in to take care of a patient for ten to fifteen minutes so that the primary nurse can leave the bedside to participate in a debrief
- This involves a change in the culture with buy in from the entire labor and delivery team
- This program looks at systems, processes, teams, and communications
- It offers a way to analyze and reflect on care in an objective manner
- In a debrief, it is important for participants to believe that they will not be punished, embarrassed, or suffer from negative consequences by asking questions, raising concerns, reporting errors, and/or offering suggestions
- It is a way to replace the older and hierarchal Morbidity and Mortality committee reviews
- At the beginning of each debrief, delegate a recorder
- Provide the second page of the INFO Debrief Tool (see below)
- The goal is to have each debrief limited to ten to fifteen minutes
- It is important to keep within the established time limits
- This shows participants that their time is valued
- It builds trust that the debrief will be as short as promised
- Also helps to ensure that participants are willing to participate in the future
- Delegate a timekeeper
- Timekeeper role is very important
- Ask for an alert at the eight minute mark and try to start wrapping the session up
- If the conversation is still rich, continue talking
- Ask for a second alert at the thirteen minute mark
- It is now time to conclude
- If there is value in continuing the conversation, the unit's director can help coordinate
- It is now time to conclude
- Report all immediate safety concerns
- Follow up with the unit director as needed
- A clinical debrief can be an effective way to identify clinicians who may need more emotional support
- Clinical Incident Stress Debrief available through Human Resources
- Referrals available for Employee Assistance Program
- A clinical debrief can be an effective way to identify clinicians who may need more emotional support
- Follow up with the unit director as needed

Once oriented, charge nurses were encouraged to start debriefing.
The debriefing champion then used modified PowerPoint presentations, specific to each discipline, to introduce the project to the labor and delivery nurses, Neonatal Intensive Care Unit nurses, Neo/Peds Respiratory Therapists, and to the OB/GYN department. Participants were encouraged to start debriefing as needed.
The same survey, with two additional questions about practice change, was distributed at the six month point into the pilot. A third, and final survey about clinician’s knowledge, skills, and attitudes about debriefing after critical obstetric events will be distributed exactly one year after debriefing was introduced on the clinical unit.
In addition, a Debriefing Committee has been formed to follow up with the feedback and recommendations recorded during the debriefs. The committee meet monthly to not discuss and implement the recommendations, but also to focus on the continual promotion of this program and celebration of successes. A list of actions is being documented to collect objective data about changes that have been implemented secondary to debriefing.
The debriefing champion then used modified PowerPoint presentations, specific to each discipline, to introduce the project to the labor and delivery nurses, Neonatal Intensive Care Unit nurses, Neo/Peds Respiratory Therapists, and to the OB/GYN department. Participants were encouraged to start debriefing as needed.
The same survey, with two additional questions about practice change, was distributed at the six month point into the pilot. A third, and final survey about clinician’s knowledge, skills, and attitudes about debriefing after critical obstetric events will be distributed exactly one year after debriefing was introduced on the clinical unit.
In addition, a Debriefing Committee has been formed to follow up with the feedback and recommendations recorded during the debriefs. The committee meet monthly to not discuss and implement the recommendations, but also to focus on the continual promotion of this program and celebration of successes. A list of actions is being documented to collect objective data about changes that have been implemented secondary to debriefing.
